
孕与不孕之迷思




Parenting Adventures is about brutally honest discussions in the world of parenting. In this sixth episode, we explore the subject of infertility. How do couples recover from the grief of knowing they may never have children? Why are they not open to the option of adopting or using a donor? We find out from a fertility specialist and, we will also hear from someone who didn’t take her infertility diagnosis as the final result, and did everything she could to become a mother.
Do click on this link to hear the podcast:
http://www.bfm.my/parenting-adventures-6-dealing-with-infertility.html

A weighty issue
How a woman’s weight impacts the risk of miscarriage
A miscarriage is a devastating experience for couples, perhaps even more so for those who have struggled with infertility and gone through the initial joy of a successful fertility treatment. Statistics have shown that in both natural and IVF conception, about one in six pregnancies will end in a miscarriage before the 20th week, with the rate being higher in older couples.
Understandably, couples are frightened of miscarriages and would rather not think or talk about it. However, it is important for couples to understand why miscarriages happen, as well as what they can do to reduce their risks.
Although the exact reason for a miscarriage is often unexplainable, it can occur due to a number of reasons. These include chromosomal abnormality, improper implantation of the egg and maternal health problems or trauma. The mother’s age also plays a significant role, as does her lifestyle, which includes exposure to stress, smoking, drug use, malnutrition, excessive caffeine, radiation and toxins.
Another well-studied factor than increases a woman’s risk for miscarriage, is her weight. As these studies indicate, if the mother is obese or underweight, this increases her risk of not only infertility, but miscarriage as well, regardless of the method of conception.

According to researchers at the Department of Obstetrics and Gynaecology, University of Adelaide, Australia, being overweight increase a woman’s risk of miscarriage by 29%, while being obese can increase the risk by 71% or more. However, for women undergoing assisted reproduction, researchers at the Assisted Fertilization Center, Brazil concluded that maternal obesity could increase the risk of miscarriage by up to 1330%.
Obesity also compounds miscarriage rates in women with PCOS. The Department of Obstetrics and Gynecology, Faculty of Medicine, Erciyes University, Turkey found that the miscarriage rate in obese women with PCOS is about nine times higher than average.
And while miscarriage is often the result of an unhealthy fetus, researchers from the Department of Obstetrics and Gynecology, Stanford Hospital and Clinics, CA, USA found that the risk of miscarriage of a healthy fetus is significantly higher in obese women (with BMIs of 25 or more).
While obesity has been identified as a risk factor for spontaneous miscarriage, the mechanism for it remains unclear. But a study by The Academic Unit of Reproductive and Developmental Medicine, The University of Sheffield and Sheffield Teaching Hospitals, Sheffield, UK points to the endocrinological changes in obesity as possibily causing complex adverse effects including circulating adipokines, sex steroids and insulin resistance.
Women who are underweight, with a BMI of under 20, also face an increased miscarriage risk. A study by researchers at the German Cancer Research Centre found that pregnant women who were underweight faced a 70 % higher risk of having a miscarriage.
Therefore, it can be concluded that among intrauterine environmental factors, nutrition appears to play the most critical role in influencing placental and fetal growth. Since maternal undernutrition or overnutrition during pregnancy can impair fetal growth, women must adopt healthier diets and incorporate exercise to lower their risk of miscarriage.
If you have any concerns regarding miscarriage, especially after IVF, please do not hesitate to consult with your fertility consultant for advice.


What you should know about PGD & PGS
If you and your partner have been struggling with fertility issues and are seriously considering In-Vitro Fertilisation or IVF, the consideration of whether you should be undergoing PGD and PGS on top of an IVF can be quite daunting. This is because, in normal IVF procedures, the best embryos are selected based on their appearance and morphology only. Therefore, the genetic content of those embryos or any chromosomal abnormality cannot be detected. However, by undergoing PGD and PGS, you will be able to screen your embryos for any potential genetic and chromosomal issues. However, before we jump into the band wagon of having PGS or PGD, there are a few things we need to consider.
What is PGS?
PGS stands for Pre-implantation Genetic Screening. In PGS, a cell is taken from an embryo which was created following an IVF procedure, so that it can be tested for chromosomal abnormalities before the embryo is transferred to the womb. This test will be able to tell us whether the embryo has normal sets of chromosomes. However, it will not be able to tell us whether this embryo has a genetic problem or not.
It is important to note that not all the patients going through an IVF required a PGS. You may want to consider it if:
The PGS procedure involves:
1. You will undergo a normal IVF treatment and your eggs will be collected and fertilised.
2. An embryo is grown in the laboratory for a few days.
3. An embryologist will perform a biopsy and remove a few cells, usually on day 3 or 5.
4. All 24 chromosomes are analysed (22 non-sex chromosomes and two sex chromosomes X & Y).
5. If the embryo is normal, it will be transferred into your womb.
6. Any remaining unaffected embryos can be frozen for later use.
7. Affected embryos will be allowed to perish.


What is PGD?
PGD is an abbreviation for Preimplantation Genetic Diagnosis. In PGD, a cell is taken from an IVF embryo so that it can be tested for a specific genetic condition before the embryo is transferred to the womb. It can be used to test for any genetic condition that is known to be caused by a specific gene.
At present, PGD is used to screen for more than 250 genetic conditions, such as Huntington’s disease, Cystic fibrosis, Thalassaemia, Duchenne muscular dystrophy and Fragile-XPDG to name but a few. Therefore, PGD enables individuals with an inheritable genetic condition to avoid passing it on to their children. The PGD process is more tidious and challenging compared to PGS. It is used to test for a specific genetic disease which is known to your family, i.e. you or your partner is confirmed a carrier of a specific gene at a certain point of the chromosome. You need to bear in mind that by performing a PGD, it does not mean that screening of ALL genetic diseases are performed at the same time. This is because human beings have millions of gene and it is impossible to screen ALL of the genes in one go.
However, not all IVF patients need to undergo PGD. You may want to consider it, or your specialist may recommend it to you if:
• You or your partner (or both) are carriers of single gene mutations.
• You ended a previous pregnancy due to a serious genetic condition.
• You have a child with a serious genetic condition.
• Either of you has a family history of a serious genetic condition or chromosome problems.
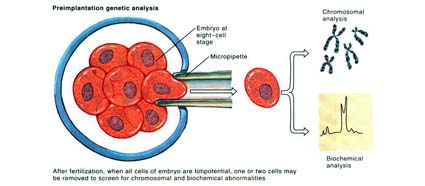
The PGD procedure involves
1. You will undergo a normal IVF treatment and your eggs will be collected and fertilised.
2. An embryo is grown in the laboratory for a few days, until it has divided into around 8 cells.
3. An embryologist will remove one or two of the cells from the embryo.
4. The cells are tested to see if the embryo has a gene that causes a genetic condition.
5. If the embryo is free of any genetic condition, it is transferred to the womb.
6. Any remaining unaffected embryos can be frozen for later use.
7. Affected embryos will be allowed to perish.
Since PGD and PGS help detect genetic conditions and chromosomal abnormalities, they help IVF patients to decide if they wish to continue with pregnancy.
The Pros and Cons of PGD and PGS
Before you decide on undergoing PGD or PGS, your fertility consultant will explain their pros and cons to you, which include:
Pros
Cons
If you and your partner are interested in or have any concerns about PGD and PGS, be sure to speak to your fertility specialist to address concerns, inquiries and options.







Like most Fertility Specialist, we faced patients with all kinds of fertility problems everyday. One of the most unique group of patients would be those who are categorised as unexplained subfertility.
It is the most frustrating & awful diagnosis for the patients. These patients are generally well but frustrated. The label of unexplained subfertility is a diagnosis of exclusion, which means that these patients had gone through most of the tests for subfertility and all the tests came back with normal results, but yet they are not able to get pregnant naturally.
In general, up to 10-25% of couples will not find any causes for their subfertility after going through fertility testing. This diagnosis can be frustrating as many of them would wonder: why is it they have not achieved a pregnancy given that all the test results had been normal?
The important thing to note is that even though all the tests are normal, it does not mean that there are no factors that prohibit them from having a baby naturally.
It is important to note that most of the fertility tests are mainly simple fertility tests. These tests do not necessarily assess function.
For example, despite showing both of your Fallopian tubes are patent through a dye test (hysterosalpingography, HSG) or a diagnostic laparoscopy, it does not necessary translate that the Fallopian tubes function are good and it does not necessarily ensure normal transport of eggs and sperm in the Fallopian tubes as there has not been a valid test for this. We know that Fallopian tubes were lined with multiple fine hairs (cilia) within the tubes, and the function of these fine hairs is to transport the eggs and sperms to meet at the most suitable place to encourage fertilisation. The cells in the Fallopian tubes also produce secretions to encourage the process of fertilization. Although the Fallopian tubes were patent, if these functions of the Fallopian tubes were poor, fertilization fails to occur. Unfortunately, there are still no tests for these conditions.
There are also conditions whereby there are poor quality of eggs or poor functionality of the sperms which attributes to this diagnosis. As Fertility Specialists, we can visualized the number of eggs you have and measure the hormones which governs egg productions. However, there is no valid test to check the quality of the eggs until the day one goes through an IVF (in-vitro Fertilization) where the doctors and the embryologists would be able to examine the eggs under microscope. Therefore, apart from being a treatment, IVF can be a diagnostic tool in its own right.
The same principle applies to the functionality of the sperms. During semen analysis, we can see the number, the activity, speed and shapes of the sperms. However, there is no test to check whether the sperms can fertilize eggs until the day we perform an IVF using these sperms. Again, IVF becomes a diagnostic test in this scenario.
If you had been diagnosed with unexplained subfertility, my advice to you would be not to leave it for ‘nature to take its course’. There maybe other underlying conditions whereby the current fertility tests available are unable to address the issues or to diagnosed the condition. It is important to put things into perspective and move on with Fertility Treatment.

