
Question: I am current 40 years-old and would like to know what is my chance of getting pregnant with IVF. Can I choose the gender of my baby when I go through an IVF
Dr Helena’s Answer:
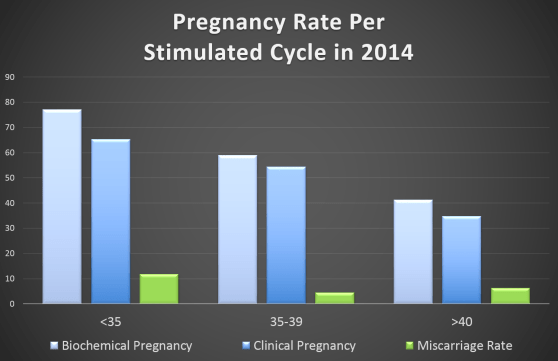
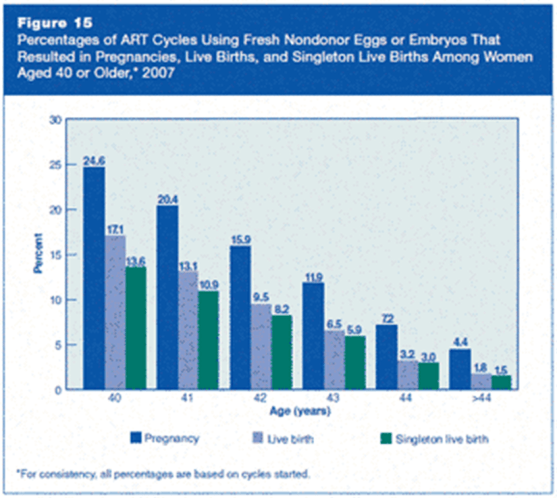
One of the biggest single determining factor for IVF success is the woman’s age. Before the age of 35, the IVF success rate is around 60-80%. After the age of 35, the success rate drops to 40-60%. The success rates of IVF drop drastically after the age of 40 to about 20-30% and then 1-2% after 45.
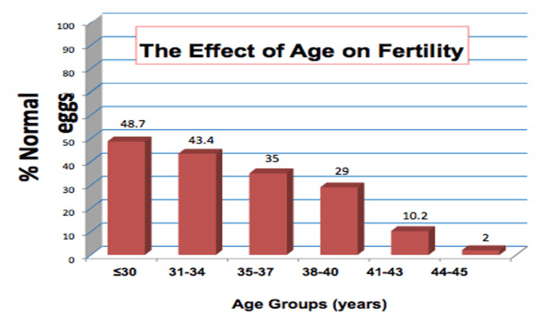
The reason for this is because as women aged, the number of follicles produce each menstrual cycle drop drastically. The quality of eggs also deteriorate as we age. As we aged, the division of chromosomes in our ovaries can become more imperfect, resulting production of eggs with faulty sets of chromosomes, leading to increase number of abnormal eggs and henceforth abnormal embryos.Therefore, women over the age of 40 has a lower rate of pregnancy with each individual IVF cycle, compare to their younger counterparts
This is a macroscopic view of the general population of women after the age of 40. However, an individual’s success rates is also dependent of her body condition, her ovarian reserves and her uterus receptivity. No two women at the age of 40 is exactly the same. A healthy 40 year-old woman with good ovarian reserves is more likely to produce good number of good quality embryos. Her counterpart who smokes and drinks, eats badly and have poor ovarian reserves is more likely to fail her IVF attempts.
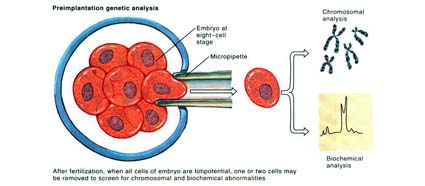
Recently, advances in Pre-implantation Screening (PGS) tests allowed us to biopsy embryos at blastocyst stage to select embryos which is normal in chromosomal make-up before embryo transfer. This test is extremely useful in determining which embryo is more likely to get our patients pregnant. However, like all the tests in this world, it comes with its problems as well. First and foremost, PGS is still expensive, and this test can only be done on embryos created from IVF, which then increase the cost of the IVF cycle. If the embryos tested showed that all the embryos are abnormal, there is no way we can change or treat these embryos and make them chromosomally normal. And therefore, some patients may end up not having any embryos which is suitable for transfer after an IVF with PGS. However, if this is the scenario, the couple can then move on quickly to another cycle of IVF to collect more embryos for PGS, hence, shortening the time required to find the ‘right’ embryo to achieve pregnancy.
Although this technology is able to reveal the gender of the embryo, one must realize that the use of such technology to perform gender selection in STRICTLY Prohibited in this country and also most countries in this world. It is important to note that IVF and PGS are technologies to help couples to achieve a healthy pregnancy and must not be misuse for ones’ whims and fancies. Science and technology should be use sensibly to maintain and restore nature’s balances and any manipulation as such can potentially tip off the balance and create potential disasters to mankind.






{kind=link}